![Adolescent Scoliosis Degrees of Curvature Chart [EXPLAINED] Image](https://clear-institute.org/wp-content/uploads/2022/08/adolescent-scoliosis-degrees-of-curvature-chart.jpg.webp)
No two cases of scoliosis are the same, which is why there is no clear-cut answer regarding its treatment needs; the very nature of scoliosis necessitates the customization of effective treatment plans. There are also different scoliosis treatment approaches that offer patients different potential results, and different severity levels.
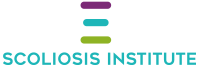
Scoliosis is a complex condition. Not only are there different condition types, but also different severity levels ranging from mild to severe. The accompanying adolescent scoliosis degrees of curvature chart shows how the two main scoliosis treatment approaches respond at each severity level.
Follow along the accompanying adolescent scoliosis degrees chart so we can explore what each severity level of scoliosis involves in terms of treatment, but first, let’s talk generally about the two main scoliosis treatment approaches.
Once a scoliosis diagnosis is given, the most important decision is how to treat it moving forward.
There are two main scoliosis treatment approaches that respond differently to the condition at each severity level: traditional and functional.
It’s important for patients, and their families, to understand the differences between the two main scoliosis treatment approaches because each offers different potential results that can have far-reaching effects.
While scoliosis is highly treatable, it is not curable, so how it’s managed throughout treatment and beyond can shape a person’s experience of life with the condition.
Scoliosis can affect all ages, but its most-prevalent form is adolescent idiopathic scoliosis (AIS), diagnosed between the ages of 10 and 18: the condition type we’re focusing on for our current purposes.
While the traditional treatment approach for scoliosis has been in place for many years, it has changed little over those years, despite our growing understanding of the condition and how it responds to treatment.
Traditional treatment is often described as reactive, while a modern functional approach, also known as conservative and/or chiropractic-centered is more proactive, which is evident in the different ways each treatment approach responds to the different severity levels.
A patient’s severity level is determined by a measurement obtained during X-ray: Cobb angle.
A patient’s Cobb angle is determined by drawing lines from the tops and bottoms of the curvature’s most-tilted vertebrae, at the apex of the curve; the intersecting angle is measured in degrees and places conditions on a severity scale of mild to severe:
Now that we’ve talked generally about the two main scoliosis treatment approaches and how adolescent idiopathic scoliosis is classified in terms of severity, let’s talk about how a scoliosis diagnosis is met, and then move on to what happens at each severity level, in terms of treatment.

In order to reach a scoliosis diagnosis, certain parameters have to be met; a person has to have an unnatural sideways spinal curve, with rotation, and a minimum Cobb angle of 10 degrees.
For both traditional and functional treatment approaches, if the above parameters are met, a diagnosis of scoliosis can be given.
Part of the diagnostic process involves further assessing and classifying conditions based on a number of important variables: patient age, causation (if known), curvature location, and condition severity.
So if adolescent idiopathic scoliosis is diagnosed with a Cobb angle measurement of between 10 and 25 degrees, how does each treatment approach respond?

Patients with mild scoliosis are advised to solely watch and wait for signs of further progression, and depending on patient age and the treatment-provider, are commonly told to return for assessment at periodic intervals every 3, 6, to 12 months.
For adolescent patients on the functional path of scoliosis treatment, mild scoliosis is responded to proactively by applying treatment as close to the time of diagnosis as possible.
Because scoliosis is progressive, we know virtually every case is going to worsen at some point, so watching and waiting while a scoliotic curve progresses unimpeded is wasting valuable treatment time.
As growth and development is the condition’s main trigger for progression, adolescents are at risk for rapid-phase progression due to the stage of puberty and its rapid and unpredictable growth spurts.
If a patient has a significant growth spurt in between scheduled assessments, this can cause the condition to progress quickly, which might have been avoidable had proactive treatment been applied earlier on.
In addition, while there are no treatment guarantees, early detection and proactive treatment applied while a condition is mild increases chances of treatment success; the treatment process is simpler while a condition is mild, the curve is smaller, more flexible, and before the body has had time to adjust to the unnatural spinal curve’s presence.
Under a functional approach, treatment of mild scoliosis involves combining therapy, rehab, scoliosis-specific exercises, and chiropractic care, while continuously monitoring for progression and adjusting treatment plans based on how the spine is responding.
If a condition progresses to the next severity level, we’re talking about moderate scoliosis, which tends to be when symptoms become more noticeable.
Cobb angle measurements of between 25 and 40 degrees are classified as moderate scoliosis, and for patients receiving traditional treatment, the only form of treatment applied is traditional bracing.
Bracing for scoliosis can be an effective facet of treatment, but only when combined with other forms of treatment so the condition is impacted on multiple levels.
The most common type of traditional scoliosis brace used is the Boston brace, which is associated with a number of shortfalls:
Fortunately, just as there are different approaches to scoliosis treatment that offer patients different potential results, there are also multiple bracing options.
For adolescents receiving functional treatment for their scoliosis, we are talking about combining multiple treatment modalities to impact scoliosis on every level.
As a CLEAR-certified scoliosis chiropractor, I see a lot of patients with moderate scoliosis because, as mentioned, this is when symptoms, like postural changes, tend to become noticeable, leading to a diagnosis and treatment.
Common postural symptoms of AIS include uneven shoulders, hips, and the development of a rib arch.

With condition-specific chiropractic care, I can apply chiropractic adjustments to the curve’s most-tilted vertebrae and work towards repositioning them back into alignment with the rest of the spine: restoring as much of the spine’s natural curves as possible.
Through applying a variety of therapies and custom-prescribed scoliosis-specific exercises, I can help patients increase their core strength so the spine is optimally supported and stabilized by its surrounding muscles.
In addition, SSEs can activate certain areas of the brain for enhanced brain-body communication, postural remodeling, and improved body positioning.
At the moderate level, I want to proactively treat conditions to prevent progressing into the severe classification level to avoid escalating symptoms and the need for more invasive treatment in the future: spinal fusion surgery.
If a patient’s Cobb angle increases into the 40+ range, this is the severe classification and is approaching the surgical-level threshold.
At the 40+ curvature-degree level, we’re talking about severe scoliosis, and for those undergoing traditional treatment, monitoring continues, bracing is likely to continue, and if unsuccessful at stopping further progression, the surgical-level threshold is crossed.
In many cases, this is when patients are funneled toward spinal fusion surgery.
While all surgeries come with their share of risks, spinal fusion is a complex, lengthy, and invasive procedure that carries some heavy potential risks and side effects:
While spinal fusion has its place in scoliosis treatment, the reality is that many cases can be treated nonsurgically.
If a patient comes to me with severe scoliosis and is wanting to forego a surgical recommendation in favor of trying a safer, more natural, less-invasive treatment option first, the focus is on stabilizing the spine and reducing the curve by integrating chiropractic adjustments, homes exercises, rehab, and corrective bracing.
To meet my patients’ bracing needs, I opt for the modern ultra-corrective ScoliBrace because it represents the culmination of what we’ve learned about the condition over the years, and how it responds to treatment.
The ScoliBrace addresses many of the shortcomings associated with the traditional Boston brace:
When combined with other forms of scoliosis-specific treatment disciplines, the ScoliBrace can augment corrective results by helping to stabilize and support the spine, while holding it in a corrective position.
At this level, we work towards reducing a curve below the surgical-threshold level to avoid the need for spinal fusion.
Part of the reason scoliosis is so often deemed a complex condition is in addition to its multiple condition types, there are also different severity levels.
The accompanying scoliosis degrees chart shows how highly variable the condition can be, ranging from mild to moderate and severe.
As a CLEAR-certified scoliosis chiropractor, I follow the CLEAR Scoliosis Institute’s treatment protocols which involves a proactive and functional treatment approach with the end goal of correction on a structural level, while preserving as much of the spine’s natural function as possible.
The traditional scoliosis treatment approach is more reactive than proactive and tends to funnel patients towards spinal fusion surgery, which has its share of potential risks and side effects.
The important thing for patients, and their families, to understand is that different scoliosis treatment approaches offer different potential outcomes, and awareness of the differences can set patients on the right path in terms of treatment outcome.

CLEAR provides a unique and innovative way of understanding scoliosis. Sign up to receive facts and information you won’t find anywhere else.